
BLUNT TRAUMA TO THE EYE
Blunt Trauma to the Eye can be due to cricket ball injury, Shuttle cock injury or even fist trauma.
Such Blunt trauma hitting the eye can cause serious internal and external injury, even when there is no open wound. The impact may lead to eyelid swelling, redness, subconjunctival bleeding, pain, blurred vision, light sensitivity, or double vision. In some cases, the force can damage deeper structures of the eye such as the cornea, lens, retina, or optic nerve.
Any eye injury from a cricket ball should be treated as urgent. Avoid rubbing the eye, do not apply pressure, and seek immediate examination by an eye specialist. Early diagnosis and treatment can prevent permanent vision loss.
RED EYES

Red eye is a common eye complaint and may occur due to infections, allergy, dryness, eyelid inflammation, bleeding under the conjunctiva, corneal infection, uveitis, or glaucoma. Some causes are mild, some are seasonal, while many can threaten vision if not treated early.
Seek urgent eye care if redness is associated with swelling, eye pain, light sensitivity, discharge, blurred vision, injury, or sudden loss of vision. Early diagnosis helps prevent complications such as corneal opacities, symblepharon, and infectious spread and protects eyesight.
Ocular External Foreign Body

Foreign bodies in the eye may include dust, sand, metal particles, glass, plastic, plant material, insects, or eyelashes. They can get stuck on the cornea, conjunctiva, under the upper eyelid, or in the lower eyelid fold, causing pain, redness, watering, irritation, light sensitivity, and blurred vision along with infection.
Do not rub the eye or try to remove a deeply embedded particle by yourself. If discomfort persists, or if there is pain, redness, watering, or blurred vision, visit an eye specialist immediately. Early removal and treatment help prevent corneal infection, scarring, and vision loss. It can be removed in most patients in a painless manner without any further complications.
Eye Lid Swellings
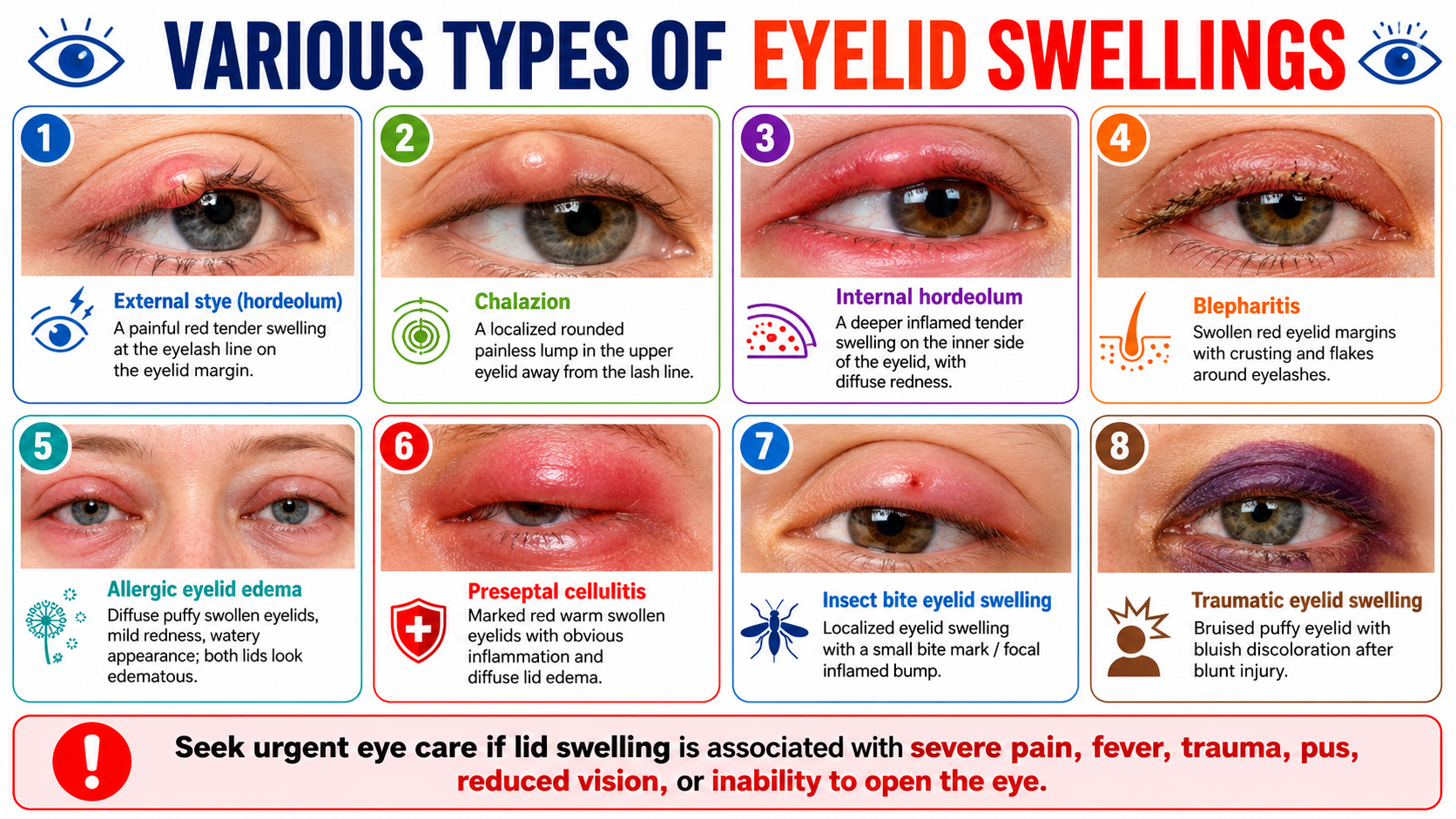
Eyelid swelling can occur due to stye, chalazion, blepharitis, allergy, insect bite, trauma, or infection such as preseptal cellulitis. It may present as a painful red bump, painless eyelid lump, crusting around lashes, puffiness, bruising, or diffuse swelling of the eyelids.
Do not squeeze or rub the swelling. Seek urgent eye care if eyelid swelling is associated with severe pain, fever, pus, trauma, reduced vision, or inability to open the eye. Early diagnosis helps prevent spread of infection and protects vision. While most swellings can be treated medically, some swellings like Chalazion may require minor sugical procedures like Incision and Curettage. Hence it is important to consult your Ophthalmologist and submit yourself to a Eye Examination.
Eye manifestations of Untreated Thyroid Disease
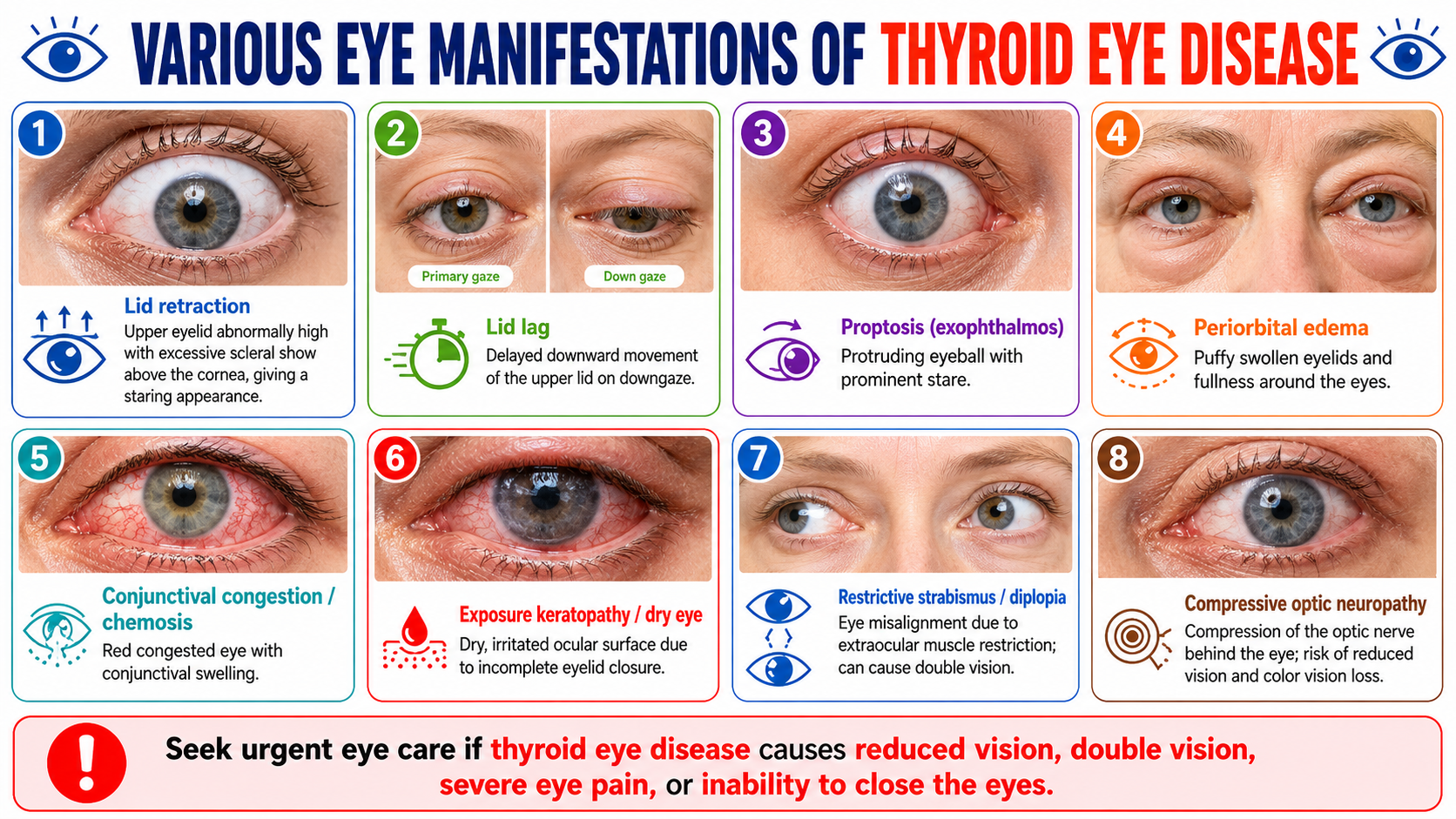
Thyroid Eye Disease, also called Graves’ orbitopathy or thyroid-associated ophthalmopathy, is an autoimmune condition in which the body’s immune system attacks the tissues around the eyes. This leads to inflammation and swelling of the eye muscles, eyelids, fat, and soft tissues inside the orbit. It is most commonly seen in patients with Graves’ disease and hyperthyroidism, but it can also occur in patients with hypothyroidism, especially autoimmune hypothyroidism such as Hashimoto’s thyroiditis, and rarely even in people with normal thyroid hormone levels.
In thyroid eye disease, the tissues behind the eyeball become inflamed and swollen. This can push the eye forward, make the eyelids retract, and prevent the eyes from closing completely. Patients may notice a staring appearance, bulging eyes, dryness, watering, redness, swelling around the eyes, pain behind the eyes, light sensitivity, or double vision. In advanced cases, swelling behind the eye can compress the optic nerve and cause reduced vision or loss of colour vision.
The most common signs include lid retraction, where the upper eyelid appears pulled up, exposing more white part of the eye; lid lag, where the eyelid does not move down normally when looking down; and proptosis, where the eyeball appears prominent or bulging. Patients may also develop eyelid puffiness, conjunctival redness, chemosis, dry eye, corneal exposure, restricted eye movements, squint, and double vision.
Dryness is very common because the eyes may not close properly during blinking or sleep. This exposes the cornea and can lead to irritation, burning, foreign body sensation, watering, recurrent redness, and blurred vision. If untreated, severe exposure can result in corneal ulceration or scarring.
Double vision occurs when the inflamed and enlarged eye muscles become stiff and restrict eye movement. This can affect reading, driving, walking, and daily activities. In severe cases, optic nerve compression can occur, which is a vision-threatening emergency.
Hyperthyroidism, especially due to Graves’ disease, is the most common thyroid condition associated with thyroid eye disease. Eye involvement may begin before, during, or after the diagnosis of thyroid disease. Sometimes the patient may have mild eye symptoms that are ignored as allergy, dry eye, or tiredness.
A baseline eye examination at the time of diagnosis helps detect early signs such as lid retraction, lid lag, mild proptosis, dry eye, reduced eye movement, early corneal exposure, or subtle optic nerve involvement including Glaucoma. Early diagnosis allows timely treatment with eye drops, control of inflammation, protection of the cornea, lifestyle advice, and proper monitoring.
Patients with Graves’ disease are commonly advised to have an ophthalmology assessment because early signs of thyroid eye disease may be missed until the condition becomes more advanced.
Many people think thyroid eye disease occurs only in hyperthyroidism. However, thyroid eye disease can also occur in people with low thyroid levels, particularly when hypothyroidism is autoimmune in origin. The immune system, not just the thyroid hormone level, plays an important role in the eye disease. The American Thyroid Association notes that thyroid eye disease is most common in Graves’ hyperthyroidism but can rarely occur in patients with normal or low thyroid levels.
Hypothyroid patients may also develop eyelid puffiness, dry eyes, ocular surface irritation, or swelling around the eyes. In some patients, early thyroid eye disease can be subtle and may not be noticed without a proper eye examination. Therefore, an eye check-up at diagnosis of hypothyroidism is useful to document baseline eye status, detect autoimmune eye involvement early, and differentiate thyroid-related eye changes from allergy, infection, dry eye, sinus-related swelling, or age-related eyelid changes.
During an eye examination for thyroid disease, the ophthalmologist may assess visual acuity, colour vision, eyelid position, eye prominence, eye movements, double vision, eye pressure, corneal dryness, conjunctival swelling, optic nerve health, and fundus status. In selected cases, imaging such as CT or MRI of the orbit may also be advised to look for enlargement of the eye muscles or optic nerve compression. Formal ophthalmology evaluation helps confirm the diagnosis and assess the activity and severity of thyroid eye disease.
Patients with thyroid disease should seek urgent eye care if they develop sudden reduction of vision, double vision, severe eye pain, inability to close the eyes, marked redness, corneal pain, increasing eye bulging, severe headache with eye symptoms, or loss of colour brightness. These may indicate active severe thyroid eye disease, corneal exposure, or optic nerve compression.
Thyroid eye disease is not just a cosmetic problem. It can affect comfort, appearance, eye movements, corneal health, and in severe cases, vision. Since it can occur with both hyperthyroidism and hypothyroidism, every patient newly diagnosed with a thyroid disorder should have a baseline eye check-up. Early detection, regular monitoring, and timely treatment can prevent complications and help protect long-term vision.
Eye Watering
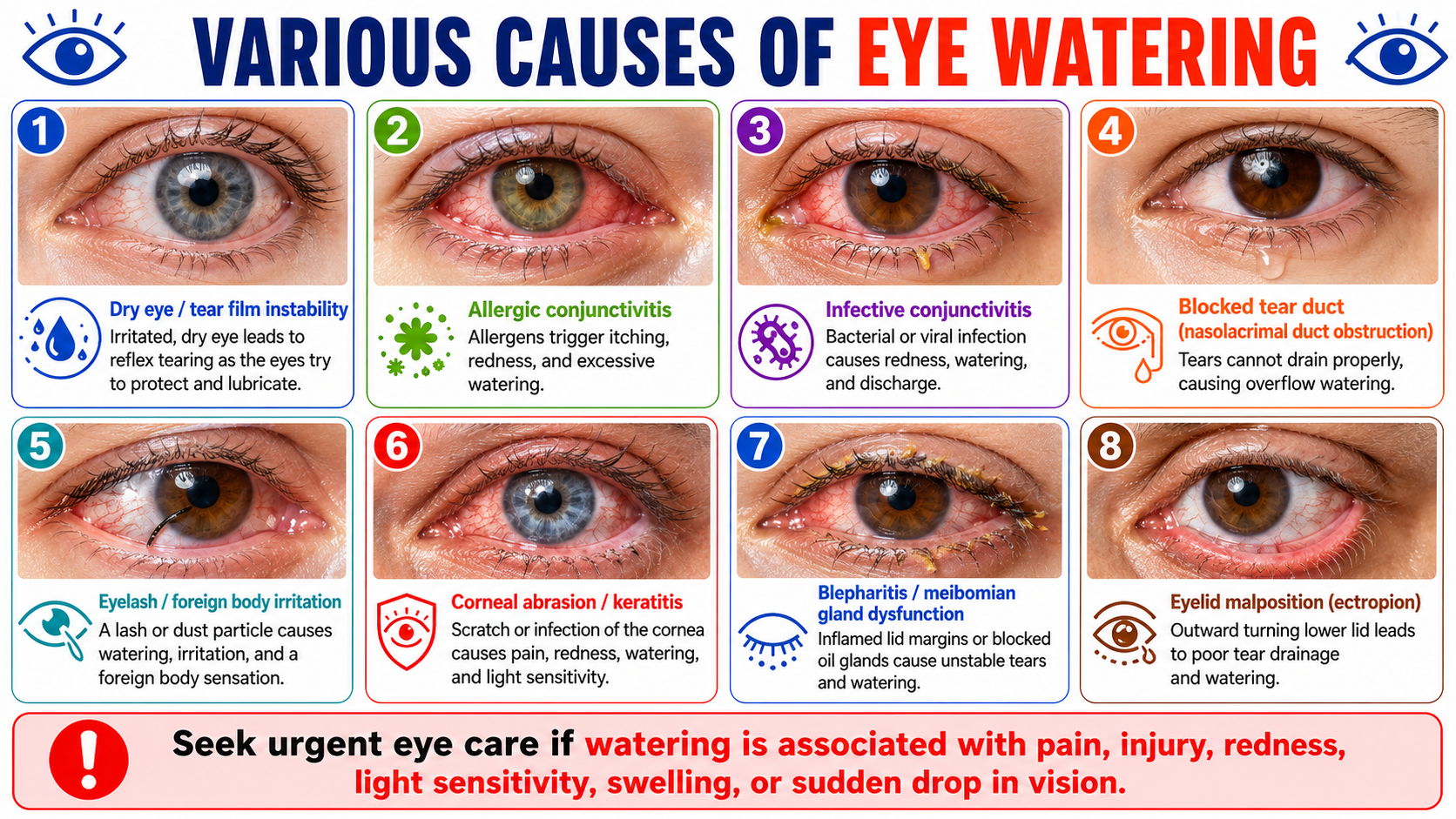
Eye watering can occur when the eyes produce excess tears or when tears do not drain properly. Common causes include dry eye, allergy, conjunctivitis, blocked tear duct, foreign body irritation, corneal injury, blepharitis, and eyelid malposition.
Persistent watering should not be ignored, especially if it is associated with redness, pain, discharge, swelling, light sensitivity, injury, or blurred vision. A timely eye check-up helps identify the exact cause and prevents complications.
Diabetic Eye Disease
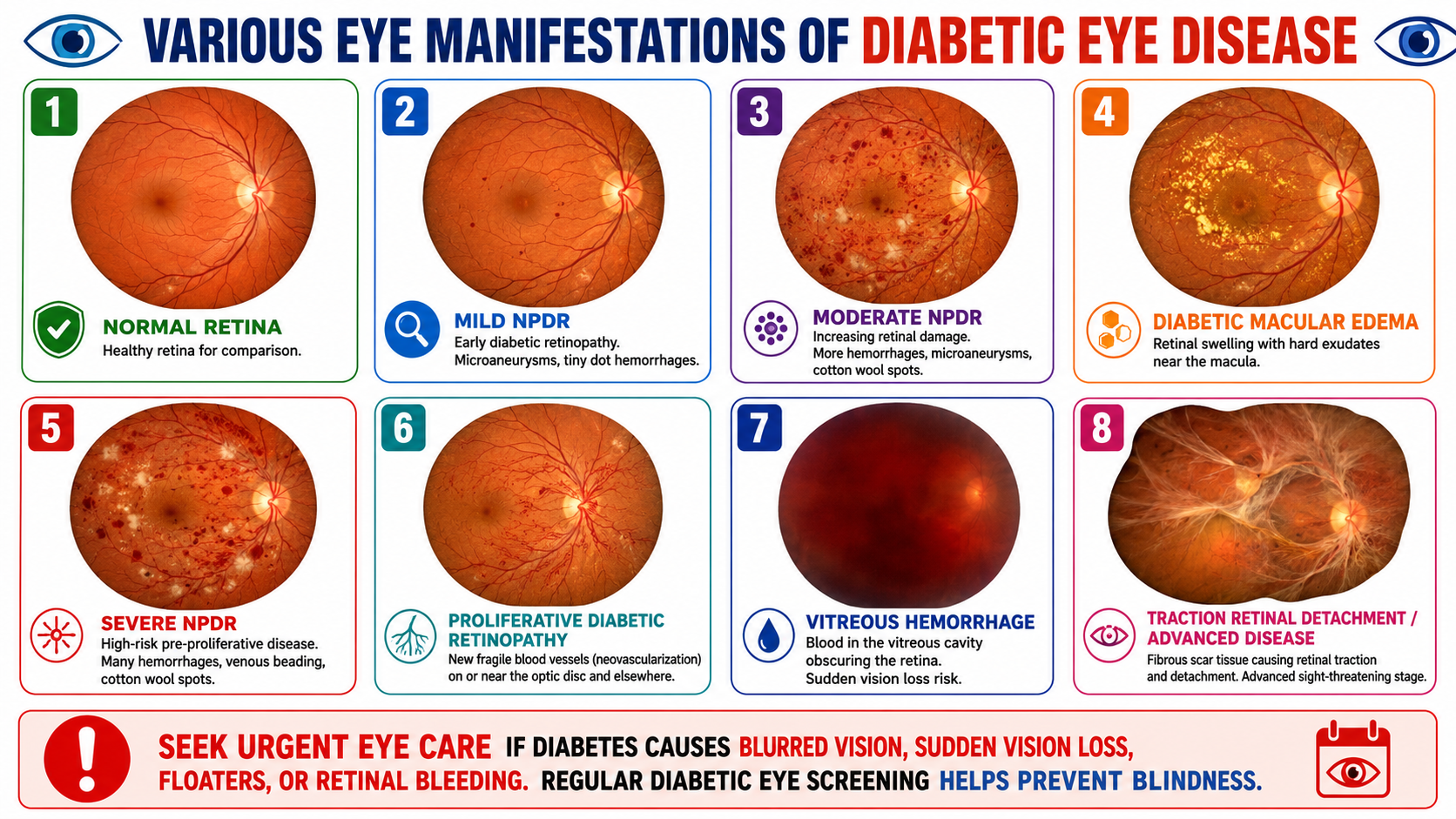
Diabetic eye disease refers to a group of eye problems that can occur in people with diabetes. The most important among these is diabetic retinopathy, a condition in which high blood sugar damages the tiny blood vessels of the retina. The retina is the light-sensitive layer at the back of the eye that helps us see clearly. Diabetes can also increase the risk of diabetic macular edema, cataract, glaucoma, vitreous hemorrhage, and retinal detachment.
Diabetic eye disease is important because it may remain silent in the early stages. A person may have retinal changes even when vision is normal. By the time blurring, floaters, dark spots, or sudden vision loss appear, the disease may already be advanced. Regular eye screening helps detect changes early, when treatment is more effective.
Long-standing or poorly controlled blood sugar weakens and damages the small retinal blood vessels. These vessels may leak fluid, blood, or fatty deposits into the retina. They may also become blocked, reducing oxygen supply to the retinal tissue.
In the early stage, called non-proliferative diabetic retinopathy, small red spots known as microaneurysms, dot-blot hemorrhages, cotton wool spots, and hard exudates may appear. As the disease progresses, more blood vessels become damaged and blocked.
In advanced disease, called proliferative diabetic retinopathy, the retina forms new abnormal blood vessels. These new vessels are fragile and can bleed into the vitreous cavity, causing sudden floaters or sudden loss of vision. They can also form scar tissue, which may pull on the retina and cause traction retinal detachment.
The macula is the central part of the retina responsible for sharp vision, reading, face recognition, and fine work. In diabetes, leaking blood vessels can cause swelling of the macula. This is called diabetic macular edema. It may cause blurred vision, distorted vision, difficulty reading, or reduced central vision.
Diabetic macular edema can occur at any stage of diabetic retinopathy and is one of the common causes of vision loss in diabetic patients.
Apart from retinopathy, diabetes can affect the eye in several ways. It can cause early cataract, fluctuations in spectacle power due to changing blood sugar levels, increased risk of glaucoma, dry eye, recurrent eye infections, and delayed healing after eye surgery or injury.
This is why a diabetic eye examination should not be limited to checking glasses alone. A complete eye evaluation is needed to assess the retina, macula, optic nerve, eye pressure, lens, and ocular surface.
An eye check-up at the time of diagnosis is especially important in type 2 diabetes, because many patients may have had high blood sugar for years before diabetes is detected. Retinal damage may already be present by the time diabetes is diagnosed. The American Diabetes Association recommends that people with type 2 diabetes should have an initial dilated and comprehensive eye examination at the time of diagnosis. (PMC)
For type 1 diabetes, diabetic retinopathy usually takes longer to develop after onset. Adults with type 1 diabetes are generally advised to have an initial dilated and comprehensive eye examination within 5 years after the onset of diabetes. (PMC)
A baseline eye check-up helps document the condition of the retina at diagnosis. It also helps the doctor decide how frequently follow-up is needed. Patients with no retinopathy may need routine periodic screening, while patients with retinopathy, macular edema, pregnancy, kidney disease, poor sugar control, or high blood pressure may need closer monitoring.
A diabetic eye check-up usually includes vision testing, refraction, slit-lamp examination, eye pressure measurement, dilated retinal examination, and fundus photography when required. Dilating drops are used to widen the pupil so that the retina can be examined properly. A dilated eye examination allows the eye doctor to look for bleeding, microaneurysms, exudates, macular swelling, new blood vessels, and retinal detachment. (Read our Webpage on Diabetic Eye Disease)
Additional tests such as OCT scan may be advised to detect macular edema. Fundus photography helps document retinal changes and compare progression over time. In selected cases, fundus fluorescein angiography may be done to study blood vessel leakage, blocked circulation, or abnormal new vessels.
Many diabetic eye changes are painless. Patients should seek urgent eye care if they notice blurred vision, sudden drop in vision, floaters, flashes of light, dark curtain-like shadow, distorted vision, difficulty reading, eye pain, redness, or sudden change in colour perception. These may indicate macular edema, vitreous hemorrhage, retinal detachment, glaucoma, or other serious complications. (MedlinePlus)
Yes. Early diabetic retinopathy may be monitored with good control of blood sugar, blood pressure, cholesterol, and regular retinal follow-up. More advanced cases may require treatment such as anti-VEGF injections, retinal laser treatment, steroid injections, or vitrectomy surgery, depending on the stage and severity.
Treatment works best when disease is detected early. Once advanced retinal damage or optic nerve damage occurs, vision recovery may be limited. Therefore, prevention and early detection are far better than waiting for symptoms.
Patients with diabetes should maintain good blood sugar control, keep blood pressure and cholesterol under control, avoid smoking, follow medical advice regularly, and attend scheduled eye check-ups. Good systemic control reduces the risk of progression, but it does not replace retinal screening.
Diabetic eye disease is a major cause of preventable vision loss. It can begin silently and progress without warning symptoms. A complete eye check-up at the time of diabetes diagnosis is essential because it detects hidden retinal changes, establishes a baseline, guides follow-up, and allows timely treatment before vision is permanently damaged.
Every person diagnosed with diabetes should consider an eye check-up as an important part of diabetes care, just like blood sugar monitoring, kidney testing, and foot examination. Regular diabetic eye screening helps protect vision and prevent avoidable blindness.
Hypertensive Eye Disease (Increased BP or Blood Pressure)
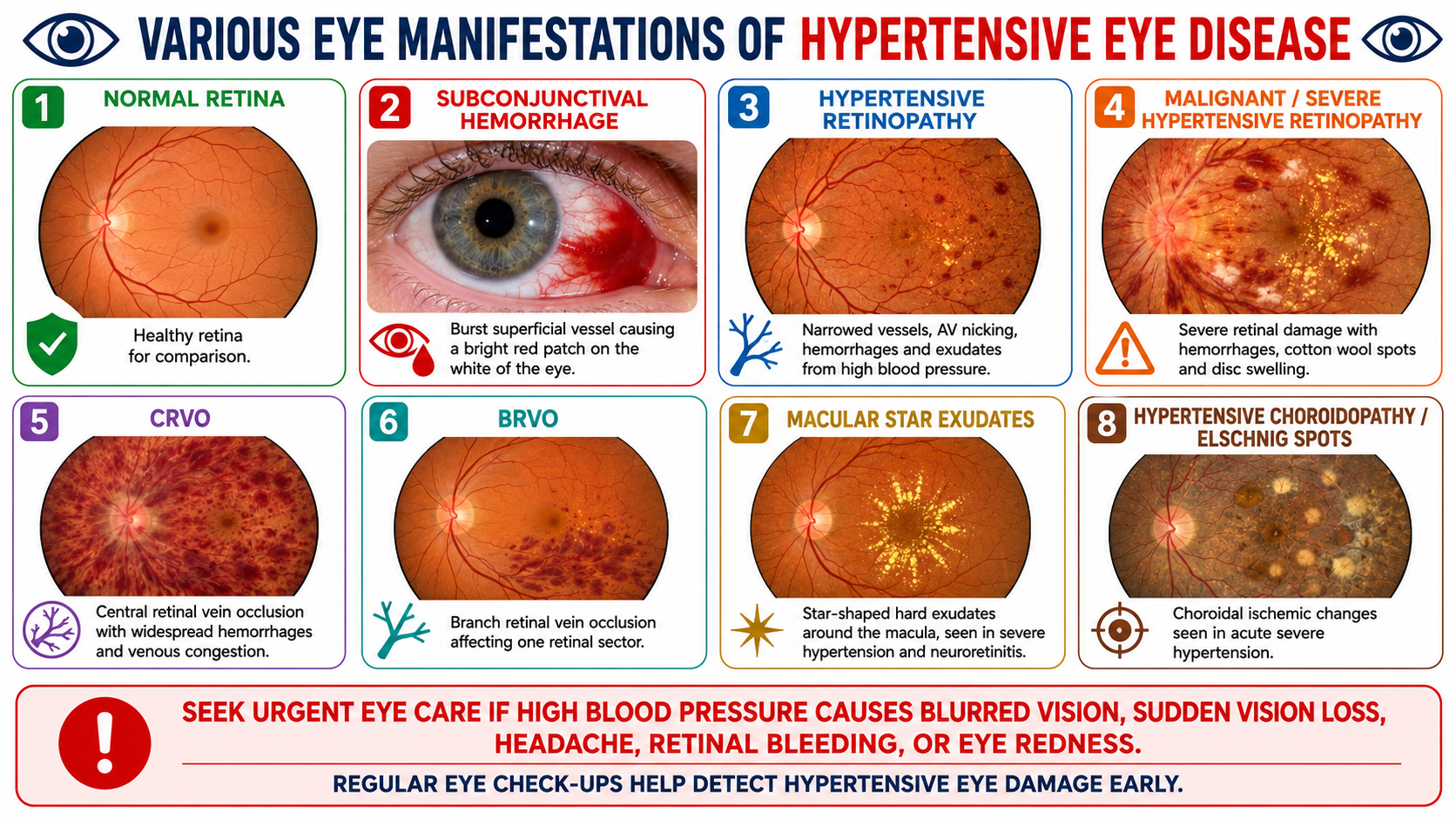
Hypertensive eye disease refers to eye changes caused by high blood pressure. The most important form is hypertensive retinopathy, where high blood pressure damages the small blood vessels of the retina. The retina is the light-sensitive nerve layer at the back of the eye that is essential for vision.
High blood pressure can also affect the choroid, optic nerve, and retinal veins. In some patients, it may lead to subconjunctival hemorrhage, retinal hemorrhages, macular star exudates, retinal vein occlusion, optic disc swelling, and even sudden loss of vision. Hypertension is considered a form of systemic target-organ damage when it affects the retina, similar to how it can affect the heart, brain, and kidneys.
The retinal blood vessels are very small and delicate. When blood pressure remains high, these vessels respond by narrowing. Over time, the vessel walls become thickened and stiff. This causes reduced blood flow, vessel leakage, and damage to the retina.
Early changes may include generalized arteriolar narrowing, focal narrowing, and arteriovenous nicking, where a thickened artery compresses a vein at crossing points. As the disease progresses, the retina may show flame-shaped hemorrhages, cotton wool spots, hard exudates, macular edema, and optic disc swelling. Key features of hypertensive retinopathy include AV crossing changes, cotton wool spots, flame-shaped hemorrhages, disc swelling, and macular star formation.
Subconjunctival hemorrhage may appear as a sudden bright red patch on the white part of the eye. It happens when a small superficial blood vessel breaks under the conjunctiva. It often looks alarming but may be painless. However, if it occurs repeatedly, or if the patient has known hypertension, blood pressure should be checked and an eye evaluation is advisable.
Hypertensive retinopathy is the classic retinal damage due to high blood pressure. Early stages may not cause symptoms, but the eye doctor can detect changes in the retinal vessels during fundus examination.
Severe or malignant hypertensive retinopathy may occur when blood pressure rises suddenly or remains dangerously high. It can cause retinal bleeding, cotton wool spots, hard exudates, macular star, optic disc swelling, and visual symptoms. This may indicate a hypertensive emergency and requires urgent medical attention.
Macular star exudates are yellow lipid deposits arranged in a star-like pattern around the macula. They may be seen in severe hypertension and other conditions such as neuroretinitis. When the macula is affected, central vision may become blurred or distorted.
CRVO, or central retinal vein occlusion, occurs when the main retinal vein is blocked. It can cause widespread retinal hemorrhages, swollen retina, dilated tortuous veins, and sudden painless vision loss. Hypertension is an important risk factor.
BRVO, or branch retinal vein occlusion, occurs when one branch of the retinal vein is blocked. It usually affects one sector of the retina and can cause blurred vision, retinal bleeding, macular edema, or floaters.
Hypertensive choroidopathy occurs when very high blood pressure affects the choroidal circulation. It may cause choroidal ischemia, Elschnig spots, Siegrist streaks, serous retinal detachment, and visual symptoms. This is more commonly associated with acute severe hypertension.
An eye check-up at the time of hypertension diagnosis is important because the retina provides a direct view of the body’s small blood vessels. By examining the retina, the eye doctor can detect microvascular damage caused by high blood pressure. The retina is one of the few places where blood vessels can be directly seen without surgery.
Many patients with early hypertensive retinopathy have no visual symptoms. They may feel that their eyes are normal, but retinal vessel narrowing or AV nicking may already be present. A baseline eye examination helps document the condition of the retina at diagnosis and helps compare future changes.
A fundus examination is also useful because hypertensive retinal changes may reflect damage in other organs. Evaluation of hypertension commonly includes looking for end-organ damage, and fundoscopy is one way to assess retinopathy or maculopathy.
Hypertension is often called a silent disease because many people do not feel symptoms until complications occur. Similarly, hypertensive eye disease may progress quietly. The patient may have normal vision even when retinal blood vessels are already affected.
A complete eye check-up can detect early vessel narrowing, AV crossing changes, retinal hemorrhages, cotton wool spots, exudates, macular edema, optic disc swelling, and retinal vein occlusions. Detecting these changes early helps the physician and patient understand whether blood pressure control is adequate and whether closer systemic monitoring is needed.
A hypertensive eye evaluation may include visual acuity testing, refraction, slit-lamp examination, blood pressure correlation, eye pressure measurement, dilated retinal examination, and fundus photography. The eye doctor examines the retina, retinal arteries, retinal veins, optic disc, macula, and choroidal changes.
In selected cases, additional tests such as OCT scan may be advised to detect macular edema or optic nerve swelling. Fundus photography helps document retinal changes and compare improvement or progression over time. If retinal vein occlusion or vascular leakage is suspected, retinal imaging and angiography may be advised.
Early detection of hypertensive eye disease allows timely blood pressure control and monitoring. Mild retinal vessel changes may stabilize or improve with good blood pressure control. However, advanced complications such as macular edema, retinal vein occlusion, vitreous hemorrhage, optic neuropathy, or retinal damage may cause permanent visual loss.
Eye findings can also alert the treating physician to uncontrolled or severe hypertension. Severe hypertensive retinopathy, disc swelling, or macular star may indicate a serious systemic situation that needs urgent medical care.
Patients with high blood pressure should seek urgent eye care if they develop sudden blurred vision, sudden loss of vision, new floaters, flashes of light, eye redness with pain, severe headache with visual symptoms, double vision, dark curtain-like shadow, or distortion of central vision.
Sudden vision loss may be due to retinal vein occlusion, retinal bleeding, macular edema, optic nerve involvement, or severe hypertensive retinopathy. These conditions should not be ignored.
Patients with hypertension should maintain good blood pressure control, take medicines regularly, reduce salt intake as advised, manage diabetes and cholesterol, stop smoking, exercise as permitted by their physician, and attend periodic eye check-ups. Eye examination does not replace blood pressure treatment, but it helps detect the effects of blood pressure on the eye and retina.
Hypertensive eye disease is an important and sometimes silent complication of high blood pressure. It can cause retinal vessel narrowing, bleeding, exudates, macular swelling, vein occlusion, optic nerve swelling, and vision loss. Since many early changes do not cause symptoms, a baseline eye check-up at the time of hypertension diagnosis is very important.
A timely eye examination helps detect retinal damage early, document the baseline status, guide follow-up, and alert the patient and physician to possible systemic risk. Regular eye check-ups, along with good blood pressure control, help protect both vision and overall health.
Glaucoma
Glaucoma is a group of eye diseases that damage the optic nerve, the nerve that carries visual signals from the eye to the brain. This damage is often related to increased eye pressure, also called intraocular pressure, but glaucoma can sometimes occur even when eye pressure is within the normal range. If untreated, glaucoma can lead to permanent vision loss and blindness.
Glaucoma is commonly called the silent thief of sight because most patients do not notice symptoms in the early stages. Vision loss usually starts from the sides, affecting peripheral vision first, while central vision may remain clear until the disease becomes advanced. Because the early damage is painless and gradual, many people come for treatment only after significant optic nerve damage has already occurred.
Inside the eye, a clear fluid called aqueous humor is continuously produced and drained. If this fluid does not drain properly, eye pressure can rise. Raised eye pressure can slowly damage the optic nerve fibers. Over time, this leads to optic nerve cupping, thinning of the neuroretinal rim, retinal nerve fiber layer loss, and visual field defects.
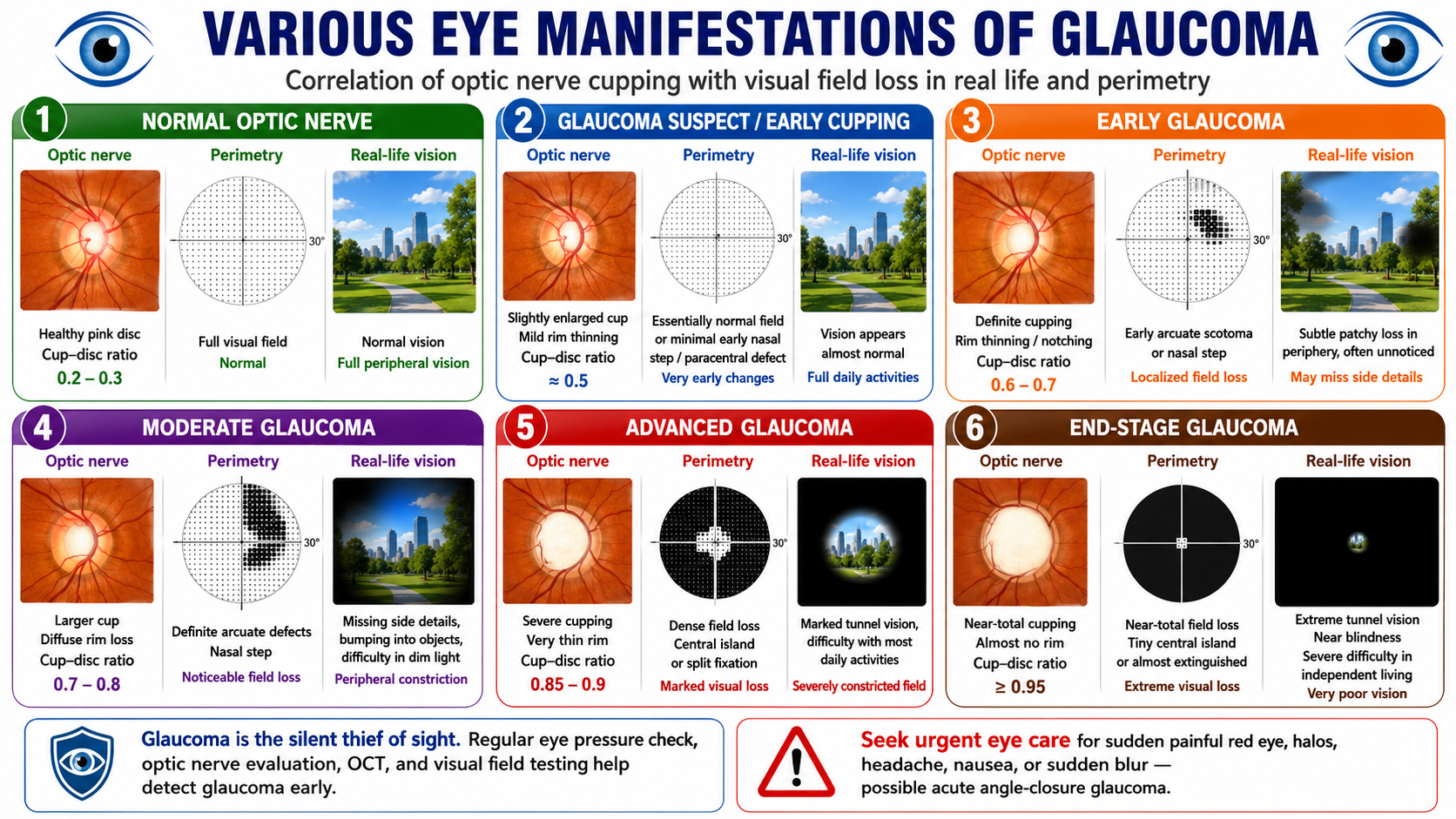
The optic nerve head has a central pale depression called the cup and a surrounding pink nerve tissue called the rim. In glaucoma, the cup gradually enlarges and the rim becomes thinner. This is called glaucomatous cupping. As optic nerve damage progresses, the patient develops corresponding defects in the visual field.
In a normal optic nerve, the cup is small and the surrounding rim is healthy. The visual field is full, and the patient has normal central and peripheral vision.
In glaucoma suspect or early cupping, the cup-disc ratio may be larger than expected, or there may be mild rim thinning. At this stage, visual field testing may still be normal or show very subtle changes. The patient usually has no symptoms.
In early glaucoma, optic nerve cupping becomes definite. There may be localized rim thinning or notching. Visual field testing may show early nasal step, paracentral scotoma, or arcuate defect. In real life, the patient may still feel vision is normal because the brain adapts and central vision remains good.
In moderate glaucoma, optic nerve rim loss becomes more obvious. Visual field defects become larger and more definite. Patients may start missing objects from the side, bump into things, or have difficulty in dim light.
In advanced glaucoma, only a small central island of vision may remain. The patient may experience marked tunnel vision and difficulty walking, reading, driving, or doing daily activities.
In end-stage glaucoma, there may be near-total optic nerve cupping and almost complete field loss. Vision may be reduced to a tiny central island or may be lost completely. Damage caused by glaucoma cannot usually be reversed, which is why early detection is extremely important.
Primary open-angle glaucoma is the most common type. The drainage angle of the eye remains open, but fluid drainage is inefficient. Eye pressure may rise slowly, and optic nerve damage occurs gradually over years. This type is usually painless and symptom-free in the early stages.
Angle-closure glaucoma occurs when the drainage angle becomes narrow or blocked. It may be chronic and silent, or it may present suddenly as an acute attack. Acute angle-closure glaucoma is an emergency and may cause severe eye pain, redness, blurred vision, halos around lights, headache, nausea, and vomiting. It requires immediate eye care to prevent permanent vision loss.
Normal-tension glaucoma occurs when optic nerve damage happens despite eye pressure being in the statistically normal range. These patients still need monitoring and treatment because the optic nerve is vulnerable.
Secondary glaucoma occurs due to another eye or body condition, such as eye injury, steroid use, inflammation, advanced cataract, diabetes-related eye disease, retinal vein occlusion, or previous eye surgery.
Congenital and childhood glaucoma occur in infants or children due to developmental problems in the eye’s drainage system. Symptoms may include large eyes, watering, light sensitivity, and cloudy cornea.
The risk of glaucoma increases with age, raised eye pressure, family history of glaucoma, thin cornea, high myopia, diabetes, hypertension, steroid use, previous eye injury, and certain anatomical eye features such as narrow angles. Some people are at higher risk even if they have no symptoms, so routine screening is important.
Most patients with open-angle glaucoma have no symptoms in the beginning. They may read normally, see faces clearly, and carry out daily activities without noticing any problem. This is because central vision is preserved until late stages.
As glaucoma progresses, symptoms may include difficulty seeing objects from the side, missing steps while walking, bumping into objects, difficulty driving at night, patchy vision loss, tunnel vision, and eventually severe visual impairment.
Symptoms of acute angle-closure glaucoma are different and sudden. They include severe eye pain, redness, blurred vision, coloured halos around lights, headache, nausea, vomiting, and sudden drop in vision. These symptoms require urgent treatment.
Glaucoma cannot be diagnosed by vision testing alone. A person may have 6/6 vision and still have glaucoma. A complete glaucoma evaluation includes several tests.
Eye pressure measurement checks intraocular pressure. High pressure is an important risk factor, but normal pressure does not rule out glaucoma.
Optic nerve examination helps assess cup-disc ratio, neuroretinal rim thinning, disc hemorrhage, and asymmetry between the two eyes.
Gonioscopy is used to examine the drainage angle and determine whether the angle is open, narrow, or closed.
OCT scan measures the retinal nerve fiber layer and ganglion cell complex. It can detect structural damage before the patient notices visual loss.
Visual field testing, or perimetry, maps the patient’s field of vision. It helps detect functional loss caused by optic nerve damage and is essential for monitoring progression.
Corneal thickness measurement, or pachymetry, helps interpret eye pressure readings because thin or thick corneas can affect pressure measurement.
The National Eye Institute notes that the only way to know whether a person has glaucoma is through a comprehensive thorough eye examination, because symptoms may start so slowly that they are not noticed.
Glaucoma-related vision loss is usually permanent. Treatment can protect the remaining vision, but it cannot restore vision that has already been lost. Therefore, early diagnosis is the key to preventing blindness. The American Academy of Ophthalmology notes that blindness from glaucoma can often be prevented with early treatment.
A regular eye check-up helps detect glaucoma before symptoms appear. It also helps identify glaucoma suspects, narrow angles, high eye pressure, optic nerve cupping, and early visual field defects. People above 40 years of age, those with family history of glaucoma, diabetics, high myopes, steroid users, and patients with previous eye injury should be especially careful about periodic screening.
The main aim of glaucoma treatment is to lower eye pressure and slow down further optic nerve damage. Treatment may include eye drops, oral medicines, laser procedures, or surgery. The choice depends on the type of glaucoma, stage of disease, eye pressure level, optic nerve condition, visual field damage, and patient-specific risk factors.
Eye drops are commonly used as first-line treatment. They reduce eye pressure either by decreasing fluid production or improving fluid drainage. Drops must be used regularly, even when the patient feels normal.
Laser treatment may be advised in selected cases. Laser trabeculoplasty may help open-angle glaucoma, while laser peripheral iridotomy is commonly used for narrow angles or angle-closure risk.
Surgery may be needed when eye drops and laser are not enough. Surgical options include trabeculectomy, glaucoma drainage devices, and minimally invasive glaucoma surgeries in selected patients.
Mayo Clinic notes that glaucoma treatment aims to lower intraocular pressure and may include prescription eye drops, oral medicines, laser treatment, surgery, or a combination of these.
Glaucoma is usually a lifelong condition. Patients need regular follow-up, repeat eye pressure checks, optic nerve evaluation, OCT, and visual field testing. Treatment should not be stopped without medical advice, even if vision appears normal.
Patients should use prescribed eye drops correctly, maintain follow-up appointments, inform family members about glaucoma screening, avoid unsupervised steroid use, and seek urgent care if sudden painful red eye or sudden vision loss occurs.
Seek urgent eye care if there is sudden painful red eye, sudden blurred vision, halos around lights, severe headache, nausea, vomiting, sudden loss of vision, or eye pain with redness. These may indicate acute angle-closure glaucoma or another serious eye condition requiring emergency treatment.
Glaucoma is a serious eye disease that can
silently damage the optic nerve and cause irreversible vision loss. In
the early stages, the patient may have no symptoms and normal central
vision, but optic nerve cupping and visual field damage may already be
developing. Regular eye pressure checks, optic nerve examination, OCT,
gonioscopy, and visual field testing help detect glaucoma early. You can
read more about it on our webpage here.
https://
Early diagnosis and timely treatment can preserve vision and prevent avoidable blindness. Glaucoma cannot be ignored, because once vision is lost, it usually cannot be regained.
UVEITIS
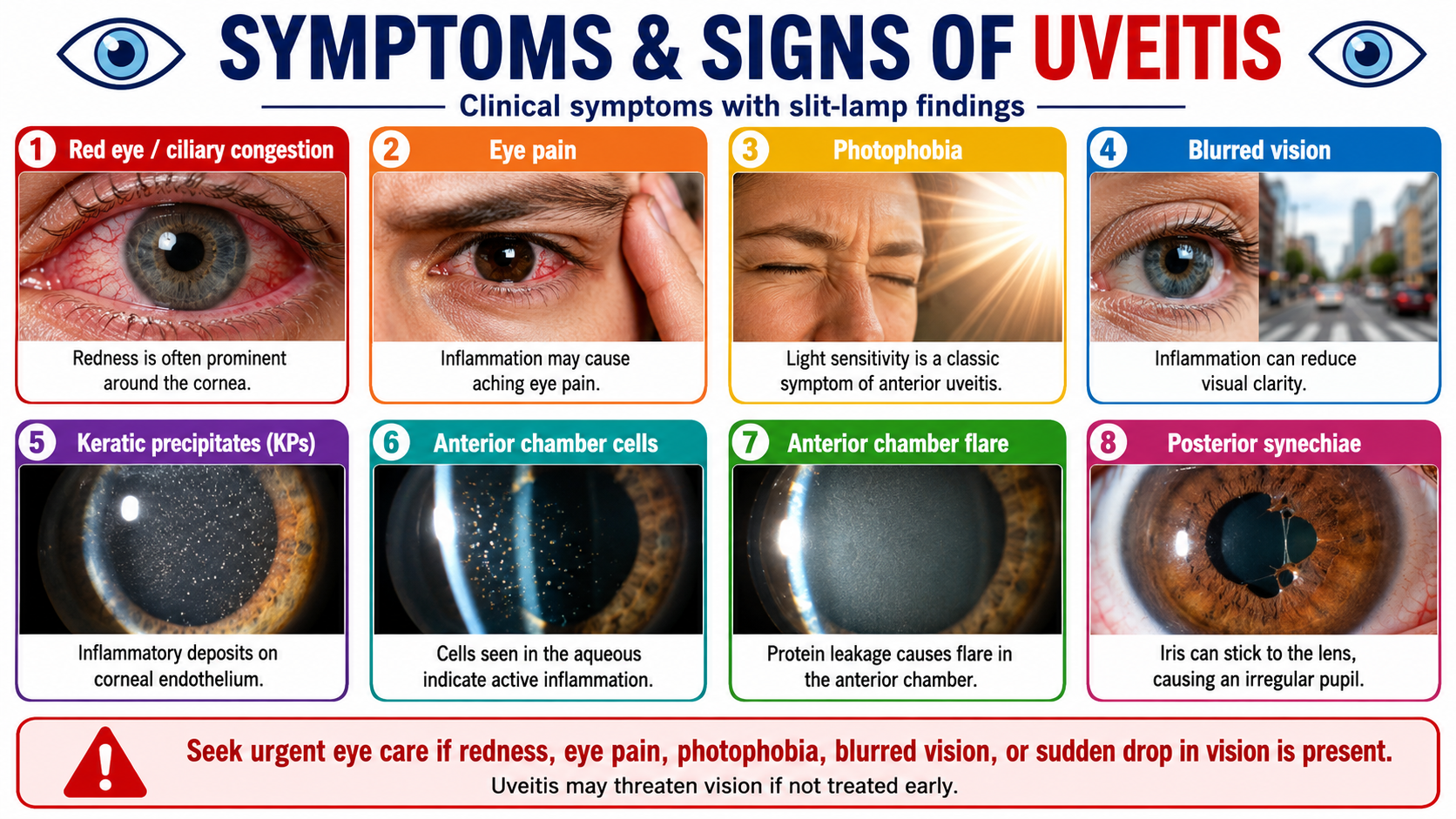
Uveitis is inflammation inside the eye and can cause redness, eye pain, photophobia, watering, floaters, and blurred vision. On slit-lamp examination, the eye doctor may see keratic precipitates, anterior chamber cells, flare, and posterior synechiae.
Uveitis should not be ignored because it can lead to cataract, glaucoma, macular swelling, retinal damage, and permanent vision loss if untreated. Seek urgent eye care if redness is associated with pain, light sensitivity, blurred vision, floaters, or sudden drop in vision.
CATARACT
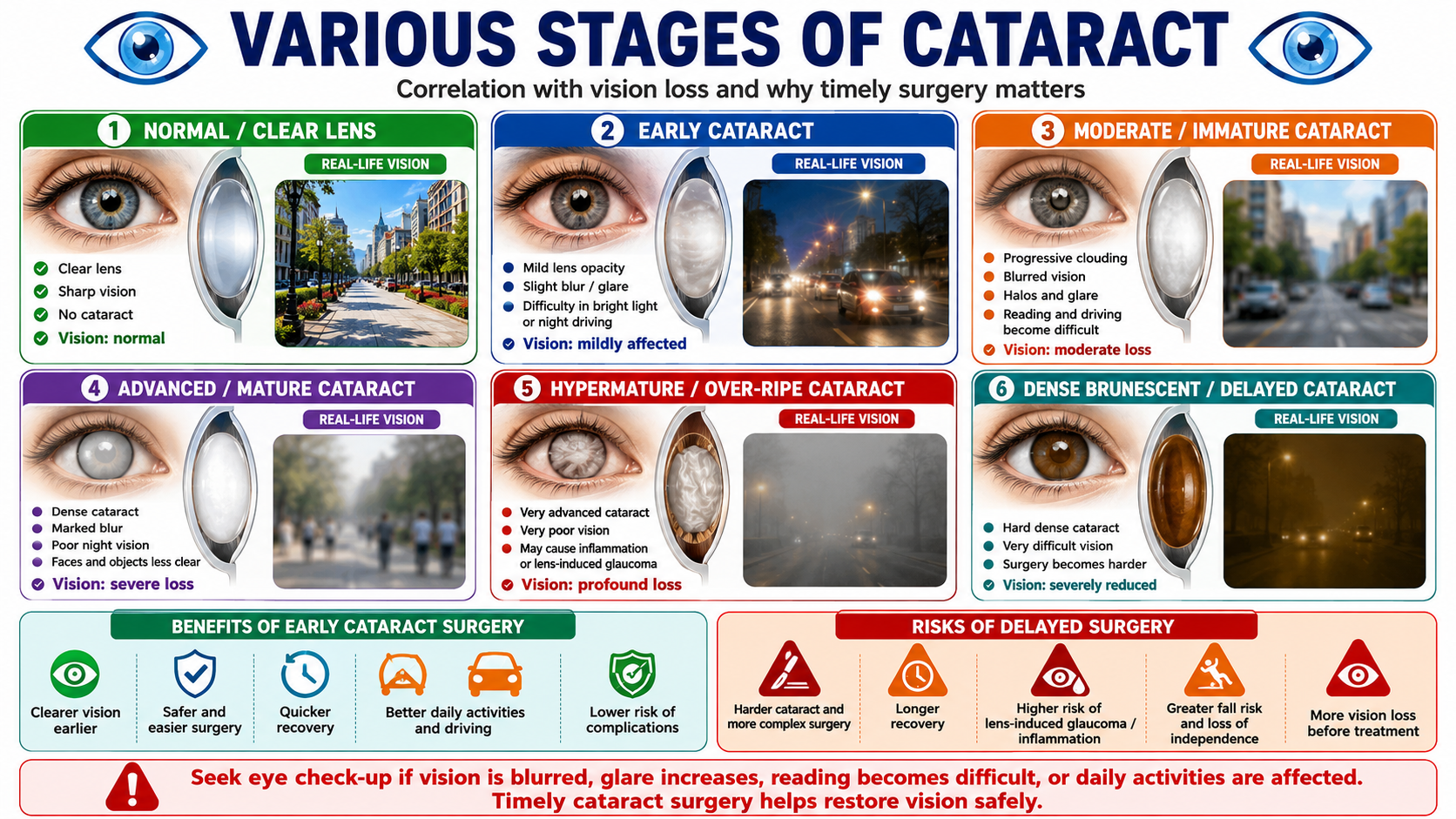
Cataract is clouding of the natural lens of the eye, causing blurred vision, glare, halos around lights, difficulty reading, poor night vision, and reduced clarity of colours. As cataract progresses from early to mature stages, vision gradually becomes more hazy and daily activities such as reading, driving, walking, and recognizing faces may become difficult.
Timely cataract surgery helps restore clear vision and is usually safer and easier before the cataract becomes too dense or over-ripe. Delaying surgery may lead to harder cataracts, more complex surgery, slower recovery, higher risk of inflammation or lens-induced glaucoma, and greater difficulty in daily life.
To know more about Cataract FAQs click here
https://
To know more about Cataract Surgery and IntraOcular lens options
including Multifocal Lens implantation. click here https://
To know more about Insurance Cashless and Reimbursement Options, click
here https://
REFRACTIVE ERRORS
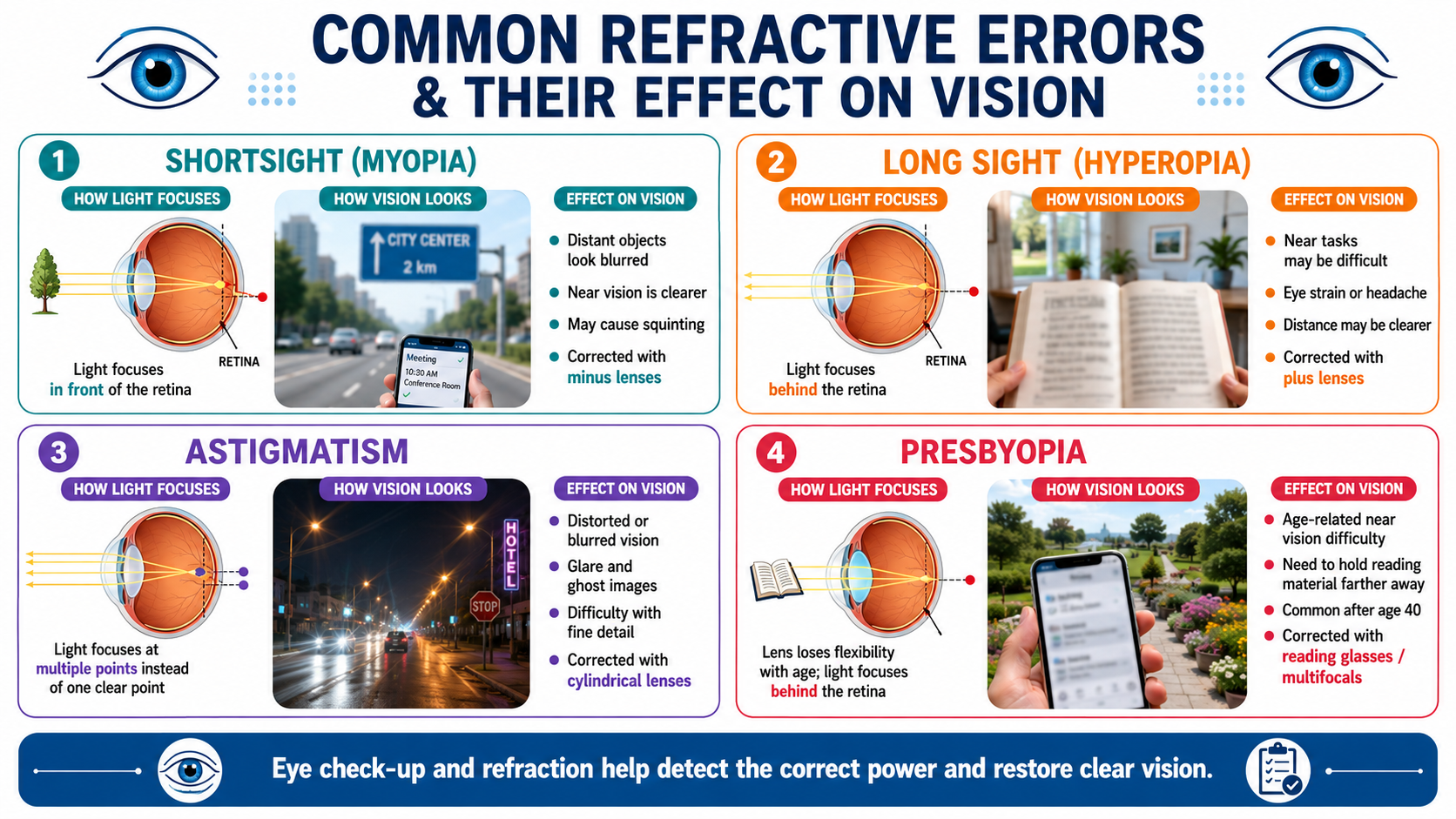
Refractive errors such as shortsight, long sight, astigmatism, and presbyopia can be corrected after a proper eye check-up and refraction test. Common treatment options include spectacles, contact lenses, reading glasses, bifocal or progressive glasses, and multifocal lenses depending on the age, lifestyle, and eye condition of the patient.
For eligible patients, advanced options such as LASIK, PRK, SMILE, ICL implantation, refractive lens exchange, or cataract surgery with premium intraocular lenses may help reduce dependence on glasses. The best treatment is chosen after detailed evaluation of corneal thickness, eye power, age, dry eye status, retinal health, and visual needs.
To know more about Refractive errors, click here
https://
To know more about Spectacle lenses, click here https://
To know more about Contact lens wear, click here https://
To Know more about Lasik FAQs, click here https://
To say Goodbye to Glasses, click here https://
To know more about Opticals at Sri Venkateshwara Nethralaya, Click here https://
Pediatric Eye Problems
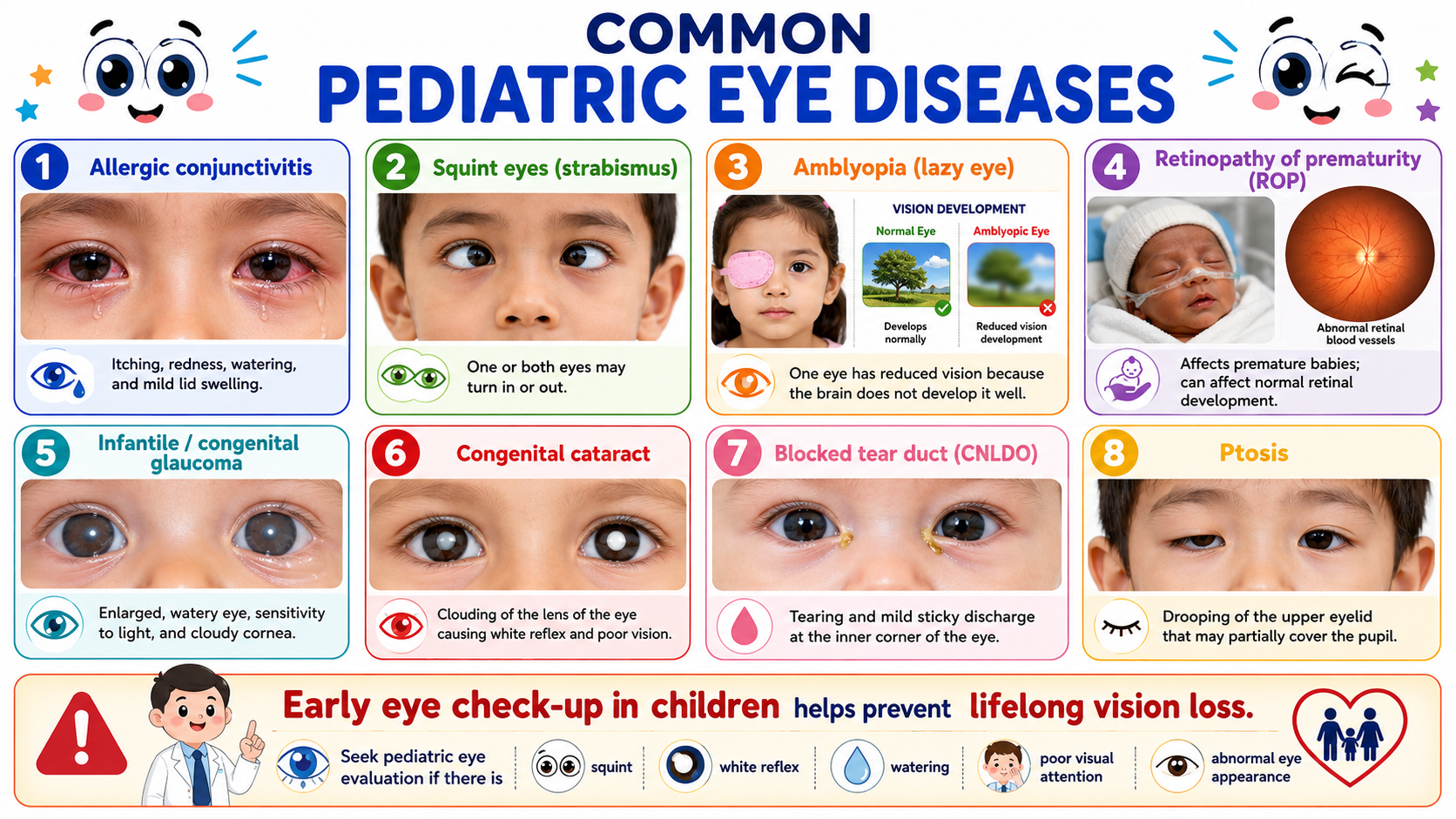
Children can develop eye problems such as allergic conjunctivitis, squint, amblyopia, retinopathy of prematurity, congenital glaucoma, congenital cataract, blocked tear duct, and ptosis. These conditions may present with redness, watering, itching, eye deviation, white reflex, drooping eyelid, cloudy cornea, poor visual attention, or delayed visual development.
Early eye examination is very important because many childhood eye diseases can affect lifelong vision if missed. Parents should seek pediatric eye evaluation if a child has squint, persistent watering, white reflex, abnormal eye appearance, light sensitivity, or difficulty seeing. Timely diagnosis and treatment can protect vision and support normal visual development.
To know more about the pediatric services at Sri Venkateshwara
Nethralaya Eye Hospital and Lasik Centre, Rajarajeshwarinagar,
Ramanagara, Kengeri Bangalore, Click here
https://
To know more about Dr Saravana Kodandapani MBBS, MD (AIIMS), Click here https://
To know more about Dr M Sukanya MBBS, DO, FIMSA, Click here https://